
Papillary thyroid cancer often requires thyroidectomy with lymph node removal due to nodal spread, while follicular thyroid cancer typically involves thyroidectomy without routine lymph node dissection, focusing on vascular invasion and distant spread risk.
Thyroid cancer is not a one-size-fits-all diagnosis. Among the most common types, papillary and follicular thyroid cancers differ not only in behaviour but also in how surgeons approach treatment. These distinctions influence the extent of surgery, lymph node management, and long-term outcomes.
Understanding these surgical differences helps patients make informed decisions, set realistic expectations, and engage confidently. Trust Dr Suvadip Chakrabarti, a trusted thyroid cancer surgeon in Kolkata, to offer clarity and peace of mind.
Today’s blog focuses on the differences between the surgical strategies for papillary and follicular thyroid cancer.
Quick takeaway: how papillary and follicular cancers differ in spread—and why that changes surgery
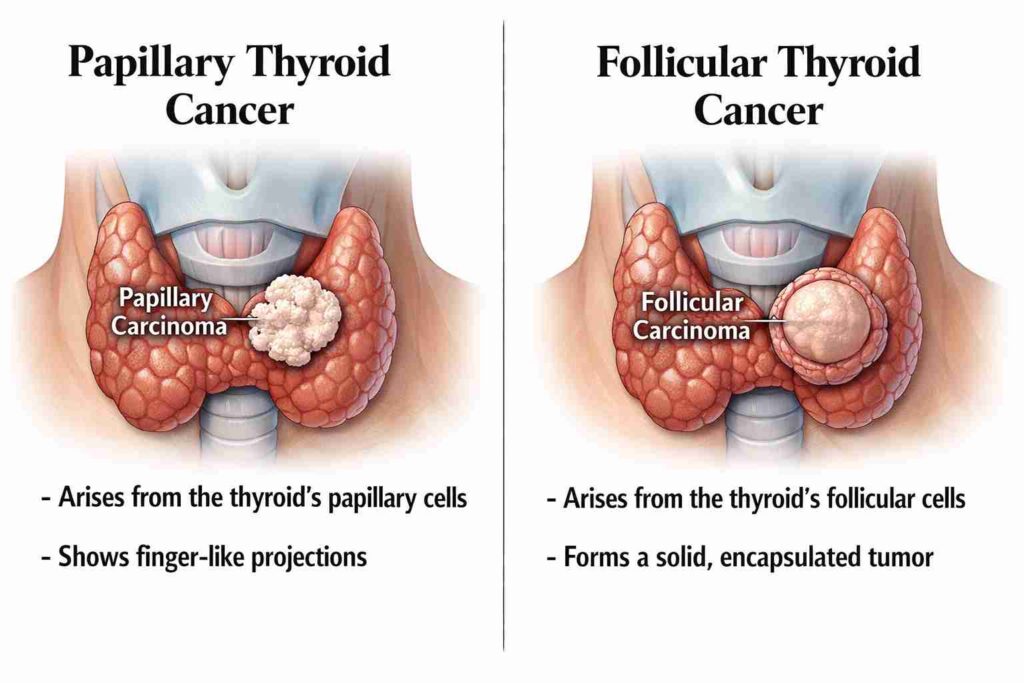
Papillary cancer spreads more through the lymph nodes in the neck. Follicular cancer spreads primarily via the bloodstream. Surgeons plan differently because the risk profile differs.
Papillary: more lymph-node tendency (neck-focused planning)
Papillary thyroid cancer often travels to nearby neck lymph nodes. That does not automatically make it aggressive, but it changes surgical thinking.
Doctors may consider:
- Careful lymph node evaluation
- Possible neck dissection if nodes are involved
- Closer ultrasound surveillance after surgery
This is why a thyroid cancer surgeon evaluates the neck as carefully as the thyroid gland itself.
Follicular: more vascular invasion/distant spread tendency (pathology-focused planning)
Follicular cancer is less likely to involve neck nodes. Instead, surgeons focus on blood vessel invasion seen on final pathology.
Key surgical concerns:
- Clear tumour margins
- Capsule invasion
- Vascular spread risk
The surgical plan depends heavily on post-resection laboratory results.
First: what “differentiated thyroid cancer” means (and why both are usually very treatable)
Differentiated thyroid cancer refers to cancers like papillary and follicular types that arise from normal thyroid cells and retain similar features.
As they grow slowly and respond well to surgery and radioactive iodine, they are usually highly treatable with excellent long-term outcomes.
Where papillary and follicular fit in the bigger thyroid cancer family
Thyroid cancers include several types, but papillary and follicular cancers account for the majority.
They are considered favourable because:
- Growth is usually slow
- Survival rates are high
- Surgery is often curative
- Additional therapy works well when needed
Early evaluation by a thyroid cancer surgeon in Kolkata improves planning and outcomes.
The diagnosis pathway that determines the surgical plan
Imaging and biopsy guide the surgery. The final plan depends on ultrasound, FNAC, and pathology risk markers.
Ultrasound + FNAC + Bethesda categories (why follicular is tricky pre-op)
Ultrasound identifies suspicious nodules. FNAC classifies them using Bethesda categories. Follicular tumours are challenging because:
- A biopsy cannot confirm invasion
- Only surgery reveals true behaviour
- Final diagnosis comes after removal
This explains why some patients need staged decisions.
When CT/MRI or laryngoscopy is used before surgery
Extra imaging is used when:
- Tumours are large
- Voice changes exist
- Extension is suspected
These tests protect nerves and guide safer surgery.
The core surgical choice: Lobectomy vs Total Thyroidectomy
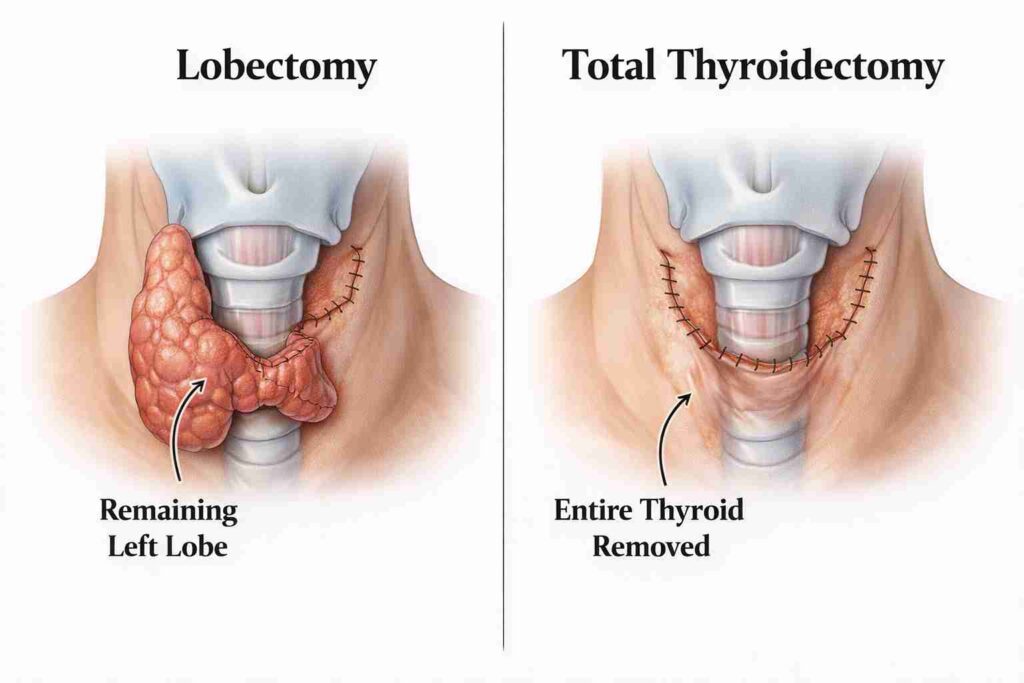
Some patients need half of their thyroid removed. Others need the entire gland removed. Risk level decides. This is the heart of thyroid lobectomy vs total thyroidectomy for thyroid cancer discussions.
When lobectomy may be enough (common low-risk situations)
Lobectomy may be considered when:
- The tumour is small
- Confined to one lobe
- No aggressive features
- No node involvement
It preserves partial thyroid function.
When total thyroidectomy is preferred (higher-risk features, bilateral disease, etc.)
Total thyroidectomy is recommended when:
- The tumour is large
- Present in both lobes
- Aggressive features exist
- Follow-up requires radioactive iodine
What “completion thyroidectomy” means and why it happens after final pathology
Sometimes, final pathology upgrades risk. Then, surgeons perform a complete thyroidectomy after a lobectomy to remove the remaining tissue.
This staged approach protects safety without overtreatment.
Neck lymph nodes: why papillary cancer more often changes the neck surgery discussion
Papillary cancer frequently affects neck nodes, so surgeons plan the neck carefully.
Therapeutic neck dissection (when nodes are proven/suspicious)
If imaging confirms nodes:
- Removal is recommended
- Disease control improves
- Recurrence risk drops
This is part of the lymph node metastasis papillary thyroid cancer surgery.
Prophylactic central neck dissection: when it’s considered—and why it’s debated
Some surgeons remove central nodes preventively. Others avoid it to reduce risk. The decision depends on tumour features and experience.
This is known as the central neck dissection papillary thyroid cancer strategy.
Why follicular cancer usually doesn’t need prophylactic lymph node surgery
Follicular cancer rarely spreads to nodes early. Therefore, routine node removal is uncommon.
Papillary vs Follicular: Surgery Impact Comparison Table
Both cancers are treated surgically, but the emphasis differs.
| Feature | Papillary | Follicular |
| Thyroid removal | Often total | Often risk-dependent |
| Node surgery | More common | Rare |
| Spread pattern | Lymphatic | Vascular |
| Pathology impact | Guides staging | Determines invasion |
After surgery: how follow-up differs (RAI, thyroglobulin, scans)
Follow-up depends on risk level and pathology findings.
When radioactive iodine is used—and when it may be skipped
Use of radioactive iodine after thyroidectomy, papillary vs follicular, depends on:
- Tumor size
- Spread
- Risk category
Low-risk patients may skip it.
TSH suppression therapy basics
Patients receive thyroid hormone to:
- Replace lost function
- Suppress cancer stimulation
Surveillance: thyroglobulin + ultrasound
Routine follow-up includes:
- Blood tumour markers
- Neck ultrasound
- Periodic scans
Risks and recovery: what patients actually experience
Most patients recover quickly. Complications are uncommon in expert hands.
Voice/nerve risk (recurrent laryngeal nerve)
Temporary hoarseness may occur. Permanent injury is rare with experienced surgeons.
Calcium/parathyroid issues
More common after total thyroidectomy. Usually temporary and manageable.
Scar, pain, hospital stay, return to work
Typical expectations:
- Small neck scar
- Mild pain
- 1–2 day hospital stay
- Return to work in 1–2 weeks
Questions patients should ask their surgeon
Informed patients make safer decisions.
- What operation are you recommending and why?
- Do I need lymph node evaluation/dissection?
- What would make you recommend completing a thyroidectomy later?
- Will I likely need RAI? What would decide that?
Dr Suvadip Chakrabarti, a notable thyroid cancer surgeon in Kolkata, explains every step clearly.
Thyroid cancer surgery in Kolkata—how to choose a centre
Choose experience, pathology quality, and nuclear medicine access over marketing.
What to look for
- High endocrine surgery volume
- Experienced pathology team
- Nuclear medicine support
What affects thyroidectomy cost in Kolkata
The thyroid cancer surgery cost in Kolkata varies by:
- Hospital type
- Surgery extent
- Node dissection
- ICU needs
Finding specialists
Finding the right specialist matters. Hospital-based endocrine teams offer coordinated care across surgery, endocrinology, pathology, and imaging, making treatment safer and more consistent compared to isolated referrals, where communication gaps can affect outcomes.
Patients across India increasingly consult Dr Suvadip Chakrabarti, a leading thyroid cancer surgeon in Kolkata, for structured, evidence-driven surgical planning.
Final Verdict:
Papillary and follicular cancers differ in their behaviour, but both are highly treatable. Surgery is customised to tumour biology, not fear. Expert evaluation ensures precise removal without unnecessary overtreatment. Care led by Dr Suvadip Chakrabarti, a reputed thyroid cancer surgeon in Kolkata, combines oncologic safety with functional preservation.
People Also Ask
Is papillary thyroid cancer less serious than follicular?
Papillary cancers are usually slower-growing, but both cancers are highly treatable with appropriate surgery.
Why did my biopsy not confirm follicular cancer until after surgery?
Follicular diagnosis requires analysis of the capsule and vessels, which a biopsy cannot fully demonstrate.
Can one avoid total thyroidectomy?
Some low-risk cases qualify for lobectomy. Final pathology decides.
Do all thyroid cancers need lymph node removal?
No. Mostly papillary cancers with node involvement require it.
When is radioactive iodine recommended?
Only in selected risk groups after pathology review.
