
Your 72-year-old mother just received a cancer diagnosis. The doctor says cancer treatment options are “complicated” because of her age.
You’re told to “wait and see.”
Meanwhile, cancer doesn’t wait. Age doesn’t pause malignancy—it amplifies vulnerability.
Cancer in older adults is not just about tumours. It is about time, strength, resilience, and the body’s true capacity to endure.
Age changes how cancer behaves, how treatment is tolerated, and how quickly complications spiral. Yet too many elderly patients are either overtreated blindly or undertreated out of fear.
The truth most families never hear?
Most elderly cancer deaths aren’t inevitable medical failures. There are consequences of dismissing age as untreatable.
Dr Suvadip Chakrabarti, the best surgical oncologist in Kolkata, refutes this claim of medical negligence, supported by evidence-based geriatric oncology protocols.
His endeavour is to transform survival statistics into living patients.
This blog breaks that dangerous middle ground with medical clarity and urgency, guided by Dr Suvadip’s oncology approach to treating older adults with cancer.
Let’s dive in.
What makes cancer treatment in older adults fundamentally different?
Cancer treatment in older adults differs because ageing affects organ function, immunity, and recovery capacity, which directly impacts treatment tolerance and outcomes. Chronological age alone should never decide treatment; biological fitness must.

(Source)
That’s severe, life-threatening, or fatal reactions in one of every two to three elderly patients receiving standard treatment. Cancer treatment for elderly patients requires precision medicine, not protocol replication.
With ageing, kidney clearance slows, bone marrow reserve declines, and healing takes longer. Older adults face higher toxicity risks if treated like younger patients without adjustment. (Source).
The danger of ignoring this reality
- Increased treatment-related mortality
- Severe treatment interruptions
- Permanent loss of independence
This is where geriatric oncology becomes non-negotiable.
Dr Suvadip Chakrabarti, the best surgical oncologist in Kolkata, integrates age-specific assessment before every treatment decision.
What is geriatric oncology, and why is it critical today?
Geriatric oncology focuses on tailoring cancer treatment for older adults based on functional age, not birth age. It balances cancer control with quality of life and independence.
Why this field exists
More than 60% of cancers occur in people above 65 (Source). Treating them with one-size protocols is medically irresponsible.
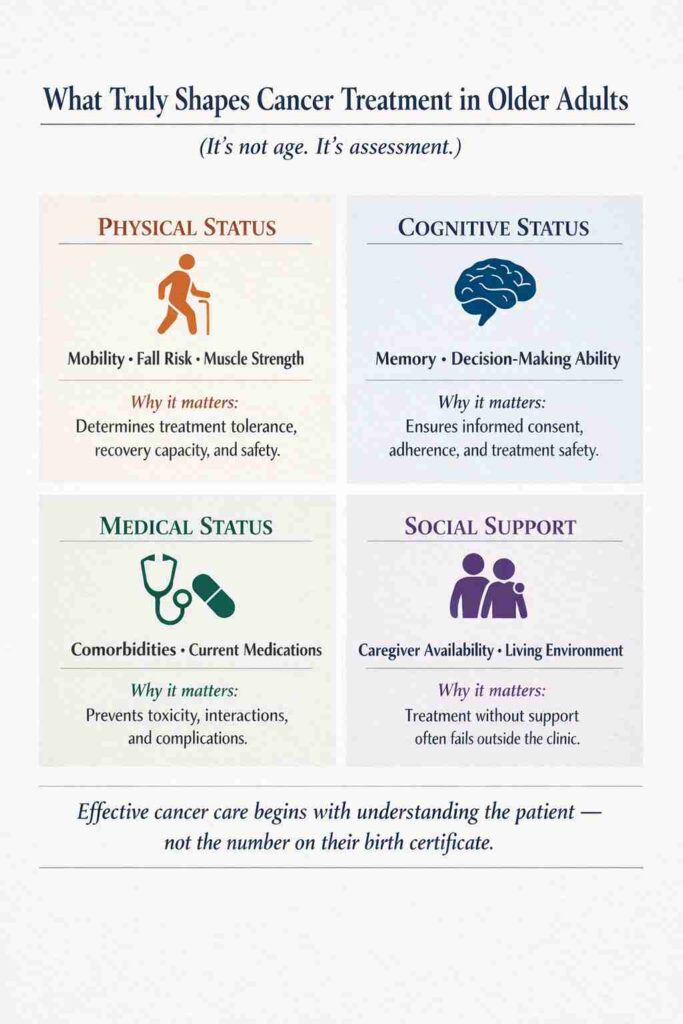
What geriatric oncology prioritises
- Functional status
- Comorbid illnesses
- Cognitive health
- Social support systems
This approach separates thoughtful oncology from reckless aggression.
How does geriatric assessment in cancer (GA / CGA) guide decisions?
Geriatric assessment in cancer (GA / CGA) evaluates physical, mental, nutritional, and social fitness to personalise treatment. It predicts treatment tolerance better than age alone.
Key components of GA
A study shows GA-guided care reduces toxicity and improves outcomes.
Why is frailty assessment in older adults with cancer essential?
Frailty assessment in older adults with cancer identifies patients at high risk of complications and treatment failure. Frailty predicts outcomes better than age or tumour stage alone.
Frailty is not weakness
It is a measurable decline in physiological reserve. Ignoring it leads to catastrophic outcomes.
Clinical consequences of missed frailty
- Chemotherapy intolerance
- Surgical complications
- Prolonged hospitalisation
This assessment protects lives, not limits care.
Is chemotherapy in older adults always unsafe?
Chemotherapy in older adults walks between cure and catastrophe.
30% to over 50% of older adult patients (age 65-70+) experience grade 3-5 (severe, life-threatening, or fatal) chemotherapy toxicities. [Source].
Dose reduction chemotherapy in elderly protocols reduces severe toxicity while maintaining efficacy.
The best surgical oncologist in Kolkata prevents chemotherapy-related side effects in the elderly by personalising every regimen based on geriatric assessment results.
Bottom line: Chemotherapy can be safe in older adults when dose, timing, and drug choice are individualised. Blind chemotherapy causes more harm than cancer itself.
Understanding elderly chemotherapy side effects
Older adults face higher risks of
- Bone marrow suppression
- Infections
- Kidney and heart toxicity
Why does chemotherapy for elderly patients matter
Evidence shows adjusted dosing maintains benefit while reducing life-threatening toxicity.
This principle follows the dose–response curve: treatment benefit plateaus at the effective dose (ED-50), while toxicity continues to rise as doses increase beyond that point.
What role does immunotherapy play in elderly cancer patients?
Immunotherapy in elderly cancer patients can be effective and better tolerated than chemotherapy in select cases. Age alone is not a contraindication for immunotherapy.
What the evidence shows
Older immune systems respond differently, but many patients benefit without severe toxicity when carefully selected.
When immunotherapy is preferred
- High chemotherapy risk
- Specific tumour markers
- Good functional status
Precision matters more than power.
How does targeted therapy for cancer in older adults change outcomes?
Targeted cancer therapy in older adults targets cancer pathways while sparing healthy cells. It reduces systemic toxicity when matched correctly.
Why targeted therapy suits older patients
- Lower collateral damage
- Oral treatment options
- Better tolerability
However, wrong selection can still cause harm. This is where experienced oncology judgment matters.
Surgery in older adults: when is it life-saving vs life-altering?
Surgery in older adults must weigh cancer control against recovery capacity and long-term independence. Well-planned surgery improves survival even in advanced age. An experienced medical oncologist in Kolkata / cancer doctor in Kolkata, works alongside a surgical oncologist to decide timing, extent, and sequencing.
Under Dr Suvadip Chakrabarti, the best surgical oncologist in Kolkata, surgical decisions are guided by biology rather than fear.
Understanding palliative care vs hospice vs supportive care
Palliative care manages symptoms alongside treatment, hospice focuses on comfort near the end of life, and supportive care spans both. Choosing palliative care does not mean giving up.
Key distinctions
| Care Type | Focus |
| Supportive | Symptom relief anytime |
| Palliative | Quality of life during treatment |
| Hospice | Comfort-focused end care |
When Should Palliative Care Enter the Conversation?
Understanding palliative care, hospice, and supportive care prevents catastrophic misconceptions. Palliative care begins at diagnosis—not death’s doorstep. It manages symptoms, reduces treatment side effects, and improves quality of life alongside curative treatment.
Hospice care is initiated when curative treatment stops and life expectancy falls below 6 months. Supportive care addresses physical and psychosocial needs throughout the cancer journey. The data stuns most families: patients receiving early palliative care live 2.7 months longer than those receiving standard oncology alone. [Source]
Early palliative care isn’t surrender—it’s strategic survival optimisation.
Why delayed decisions cost older adults the most
Delay in cancer treatment leads to rapid functional decline in older adults. Waiting narrows safe treatment options irreversibly.
Age reduces physiological margins. Every postponed decision shrinks the window for safe, effective treatment.
Why Age Deserves Precision, Not Hesitation — A Clinical Compendium
Cancer treatment in older adults requires balance, not extremes. Overtreatment without assessment increases toxicity and loss of independence. Undertreatment driven by fear reduces survival. Chronological age alone must never guide cancer decisions.
Ageing alters organ function, immunity, and recovery capacity, making standard protocols unsafe for many elderly patients. Geriatric oncology applies frailty assessment and comprehensive geriatric evaluation to personalise chemotherapy, surgery, immunotherapy, and targeted therapy.
Evidence shows individualised treatment and early palliative care reduce complications, preserve quality of life, and improve survival.
All it takes is one consultation. Book yours today!
People Also Ask
Can chemotherapy be given to elderly patients with advanced cancer?
Yes, chemotherapy can be given to elderly patients with advanced cancer if functional status, organ function, and frailty assessment indicate acceptable tolerance. Treatment goals may focus on disease control or symptom relief rather than cure.
Is there a maximum age limit for chemotherapy?
No, there is no maximum age limit for chemotherapy. Decisions are based on biological fitness, organ function, comorbidities, and frailty, not chronological age.
Can an 80-year-old receive chemotherapy safely?
Yes, an 80-year-old can receive chemotherapy safely if a geriatric assessment shows adequate functional reserve. Dose-reduced or modified regimens are commonly used to reduce toxicity.
Should an 82-year-old undergo chemotherapy?
An 82-year-old may undergo chemotherapy if the expected benefits outweigh risks based on frailty, organ function, cancer type, and treatment goals. Age alone should not determine eligibility.
Is chemotherapy safe at age 75?
Yes, chemotherapy at age 75 is often safe when treatment is individualised. Tolerance depends on physical fitness, kidney function, bone marrow reserve, and comorbid conditions.
How is stage 4 cancer treated in a 90-year-old?
Stage 4 cancer in a 90-year-old is treated with a focus on symptom control, quality of life, and selective disease-modifying therapy when tolerated. Chemotherapy may be modified or replaced with targeted or supportive care.
When is chemotherapy not recommended in elderly patients?
Chemotherapy is not recommended when severe frailty, poor organ function, uncontrolled medical conditions, or very limited life expectancy make treatment risks greater than potential benefit.
Can an 87-year-old woman be on chemotherapy?
Yes, an 87-year-old woman can be on chemotherapy if a geriatric assessment confirms sufficient functional reserve. Treatment typically involves dose adjustment and close monitoring to minimise toxicity.
