
Lymph node dissection is the surgical removal of lymph nodes near the breast to determine if cancer has spread beyond the tumour site. It’s performed when imaging or biopsy suggests cancer involvement, guiding treatment decisions and prognosis.
Women wait because they don’t know. Families crumble because no one explained that lymph nodes are not just glands—they are gates.
Once cancer enters, survival is built from surgery, chemotherapy, and faith, guided by a breast cancer surgeon who has seen outcomes most understand only when it’s too late.
Ignorance doesn’t protect you. Knowledge does. This is that knowledge.
What is lymph node dissection in breast cancer, and why is it non-negotiable?
Lymph node dissection in breast cancer is a surgical procedure used to find out whether breast cancer has spread to nearby lymph nodes, which determines the cancer stage and the next course of treatment.
It determines whether cancer has spread beyond the breast and directly influences staging, treatment decisions, and long-term survival.
The biological reality
Lymph nodes act as filters for lymphatic fluid. When cancer cells reach them, it signals that the tumour has learned to travel.
A study confirms lymph node status as one of the strongest predictors of recurrence and mortality
What this single step controls
- Cancer stage assignment
- Requirement for chemotherapy or radiotherapy
- Risk of distant metastasis
- Overall survival probability
This is not a supporting procedure. It is a decisive one.
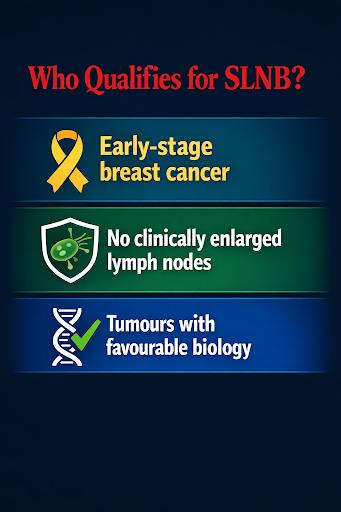
What exactly is a sentinel lymph node biopsy (SLNB)?
Sentinel lymph node biopsy (SLNB) is a surgical test used to check whether breast cancer has started spreading beyond the breast by examining the first lymph node the cancer would reach.
Furthermore, SLNB identifies and removes the first lymph node most likely to contain cancer spread, allowing accurate staging with minimal tissue damage.
How SLNB is performed
A tracer dye or radioactive substance is injected near the tumour. The first lymph node that absorbs it, the sentinel node, is surgically removed and analysed.
Large trials have shown SLNB provides accurate staging while significantly reducing complications compared to extensive node removal. Source
When does axillary lymph node dissection (ALND) become unavoidable?
Axillary lymph node dissection (ALND) is required when breast cancer has already spread to multiple lymph nodes.
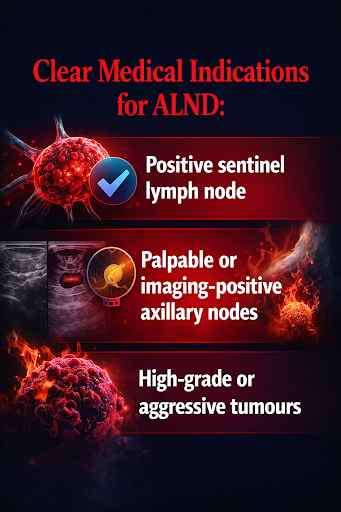
ALND removes level I and II axillary lymph nodes to reduce the risk of regional recurrence, in accordance with ASCO-endorsed protocols.
Sentinel node biopsy vs axillary dissection: what truly separates them?
Sentinel lymph node biopsy vs. axillary dissection differ in purpose: SLNB stages the disease, while ALND controls for confirmed spread.
| Parameter | SLNB | ALND |
| Nodes removed | 1–3 | 10–20 |
| Invasiveness | Low | High |
| Recovery time | Short | Prolonged |
| Complication risk | Minimal | Significant |
The decision is dictated by cancer behaviour, not surgical convenience.
Can lymph node dissection be avoided or minimised safely?
In select early-stage breast cancer cases, lymph node dissection can be safely minimised without compromising survival.
When less surgery is more medicine
Modern oncology no longer advocates maximal removal for every patient.
Multiple landmark trials confirm that limited nodal surgery is safe when cancer biology is favourable, as in the ACOSOG Z0011 Trial (formerly known as the Alliance for Clinical Trials in Oncology Z0011 Trial). Source.
Situations where node removal may be limited
- Small, early-stage tumours
- Hormone receptor–positive cancers
- No clinical or imaging evidence of node spread
Risks of unnecessary node removal
- Higher lymphedema rates
- Chronic arm pain and stiffness
- Reduced long-term quality of life
Decision balance table
| Factor | Conservative Approach | Extensive Surgery |
| Cancer control | Maintained | Maintained |
| Complications | Lower | Higher |
| Recovery | Faster | Slower |
The key lies in surgical judgment, not surgical aggression.
How many lymph nodes are removed in breast cancer surgery?
How many lymph nodes removed in breast cancer surgery depends on the procedure, ranging from 1–3 in SLNB to 10–20 in ALND. Source
Why excessive removal is harmful
A study confirms that removing additional lymph nodes does not improve survival unless cancer is present, but it dramatically increases complication rates.
How does lymph node status change breast cancer treatment planning?
Lymph node status determines cancer stage and directly dictates whether chemotherapy, radiotherapy, or extended hormonal therapy is required after breast cancer surgery.
Why lymph nodes dictate the next steps
Once lymph node involvement is confirmed, breast cancer is no longer treated as a local disease alone.
International guidelines, including those from the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO), mandate therapy escalation based on nodal burden. mandate escalation of therapy based on nodal burden. Source.
Treatment impact of lymph node findings
| Lymph Node Status | Treatment Implication |
| No nodes involved | Surgery ± hormonal therapy |
| 1–3 positive nodes | Chemotherapy often advised |
| ≥4 positive nodes | Chemotherapy + radiotherapy mandatory |
What patients must understand
- Node-positive disease increases recurrence risk
- More nodes involved = higher systemic spread probability
- Early detection of nodal spread improves survival outcomes
This is why precise lymph node assessment during surgery is not optional. It is the foundation of the entire cancer treatment strategy.
What complications can follow lymph node removal?
Lymph node removal can cause chronic swelling, pain, fluid accumulation, and functional limitations of the arm.
Lymphedema after lymph node removal
This is a chronic condition caused by impaired lymph drainage. Lifetime risk rises to 20–25% after ALND. Source.
Once established, it is lifelong.
Seroma after axillary surgery
Fluid accumulation beneath the arm is common after ALND. It can delay healing and require repeated aspiration.
Arm numbness/nerve pain after lymph node surgery
Damage or irritation of sensory nerves can result in persistent numbness, burning, or electric-shock sensations that interfere with daily life.
How does lymph node surgery affect shoulder mobility?
Without early rehabilitation, lymph node surgery can permanently limit the shoulder range of motion.
Shoulder stiffness exercises after breast cancer surgery
Targeted physiotherapy is essential and includes:
- Wall-climbing arm raises
- Pendulum movements
- Assisted range-of-motion stretches
Delayed physiotherapy increases the risk of frozen shoulder and chronic disability (British Journal of Surgery).
Why does surgeon expertise directly determine long-term quality of life
Surgical precision directly influences complication rates, nerve preservation, and functional recovery.
Choosing an experienced breast cancer surgeon in Kolkata significantly reduces avoidable harm. Dr Suvadip Chakrabarti adheres to evidence-based international protocols, employing meticulous technique and multidisciplinary coordination.
Why outcomes of breast cancer surgery in Kolkata vary so widely
Outcomes depend on the accuracy of staging, surgical judgment, and structured post-operative care.
Differences arise from inconsistent pathology support, variable access to rehabilitation, and deviation from global oncology guidelines. Under Dr Suvadip Chakrabarti, a leading breast cancer surgeon in Kolkata, patients receive integrated surgical planning, accurate staging, and continuity of care beyond the operating table.
What questions must families ask before lymph node surgery?
The right questions prevent irreversible regret and long-term suffering.
- Why is SLNB or ALND recommended in my case?
- How many lymph nodes will be removed?
- What is my personal risk of lymphedema?
- What rehabilitation plan follows surgery?
Silence here carries a lifelong cost.
This decision shapes decades, not days
Lymph node dissection is not a technical footnote in breast cancer surgery.
It has defined survival, recurrence risk, and quality of life for decades. Delay, misunderstanding, or poor surgical judgment exacts a permanent price.
People Also Ask
Does lymph node removal affect survival in breast cancer?
Yes. Lymph node status is one of the strongest predictors of survival and recurrence, as it shows whether cancer has started to spread.
Is lymph node dissection always required in breast cancer surgery?
No. Early-stage cancers may require only a sentinel lymph node biopsy if there is no evidence of metastasis.
How painful is lymph node surgery?
Most patients experience transient pain or numbness, which typically resolves with appropriate postoperative care and physiotherapy.
Can lymph node removal cause permanent arm swelling?
Yes. Lymphedema can occur, especially after extensive axillary dissection, and may be lifelong.
When should a breast cancer surgeon be consulted?
Immediately after diagnosis, before surgery decisions are finalised.
